
Psychosocial Interventions With Psychosis
本科医学论文代写 More explicitly, in the area concerned with symptom-specific approaches relating to the domain of positive symptoms such as delusions
Introduction
Psychosis is a generic phenomenon referring to the mental condition during which an individual senses a detachment from reality and realistic events around. As described by Stedman’s Medical Dictionary, psychosis can be defined as a severe mental disorder characterized by distorted personality along with loss of contact with reality in association with decline in normal social performance. It may occur with or without any evident organic damage. Individuals suffering from psychosis may report having hallucinations or delusions with split personality and disorganized communicative signals along with shambolic thinking pattern. 本科医学论文代写
This is also accompanied by reduced insight along with exhibited bizarre nature and difficulty in social communication as well as prominent impairment is observed while carrying out daily activities. A wide array of nervous system stressors can result in a psychotic reaction both at organic as well as functional level. However, the first line treatment for psychosis is generally associated with the administration of antipsychotic drugs and in some cases hospitalization, but there is increasing research evidence that suggests cognitive therapy; family therapy can be effective in the management of psychotic symptoms. This paper critically reviews on psychological intervention with patients affected by serious and prolonged mental disorders and the strengths and weaknesses associated with such types of therapeutic interventions.
译文:
介绍 本科医学论文代写
精神病是一种普遍现象,指的是个体感觉到与现实和周围现实事件脱节的心理状况。正如斯特德曼医学词典所描述的那样,精神病可以被定义为一种严重的精神障碍,其特征是人格扭曲,与现实失去联系,与正常社会表现下降有关。它可能伴随或不伴随任何明显的有机损伤而发生。患有精神病的个体可能会报告有幻觉或妄想,人格分裂和混乱的交流信号以及混乱的思维模式。
这也伴随着洞察力降低,表现出的怪异性质和社交沟通困难以及在进行日常活动时观察到的明显障碍。多种神经系统压力源可导致机体和功能层面的精神病反应。然而,精神病的一线治疗通常与服用抗精神病药物和在某些情况下住院有关,但越来越多的研究证据表明认知疗法;家庭治疗可以有效地控制精神病症状。本文批判性地回顾了对受严重和长期精神障碍影响的患者的心理干预以及与此类治疗干预相关的优势和劣势。
Psychosis
Psychosis is a mental state defining a group of mental disorders come into one singe head in psychiatry and it is characterized by certain common fundamental factors such as hallucinations or sensation of non-existent objects or phenomenon; delusions or possessing beliefs not based on reality; thought insertion, withdrawal, thought blocking, thought broadcasting lack of insight or being unable to understand the wrongs in the thinking or activity patterns. However, there are number of controversies associated with the psychiatric classification of psychosis, but usually the most common disorders come under the general title of psychoses are as follows:
- Schizophrenia
- Schizoaffective disorder
- Maniac Depression (Bipolar Disorder) 本科医学论文代写
- Mania
- Delusion (Paranoid) Disorder
- Psychotic Depression
Although these disorders differ in their symptoms but they consist of a common parameter that the individual suffering from any of the disease does not experience reality as most of the other people in general.
译文:
精神病 本科医学论文代写
精神病是一种精神状态,定义了一组精神障碍在精神病学中集中在一个单一的头脑中,其特征是某些常见的基本因素,如幻觉或对不存在的物体或现象的感觉;妄想或拥有并非基于现实的信念;思想插入、撤回、思想阻塞、思想传播 缺乏洞察力或无法理解思维或活动模式中的错误。然而,与精神病的精神病学分类相关的争议很多,但通常最常见的疾病属于精神病的总称,如下:
- 精神分裂症
- 分裂情感障碍
- 躁狂抑郁症(双相情感障碍)
- 狂躁
- 妄想(偏执)障碍
- 精神病性抑郁症
尽管这些疾病的症状不同,但它们包含一个共同参数,即患有任何疾病的个体通常不会像大多数其他人那样经历现实。
Sample Case Study
The patient is a female of 18 years doing graduation in a co-education college. She was brought to the clinic by her mother and sister for lack of sleep, verbal and physical aggressiveness, suspicion that the male faculty members in her college are writing love letters to her and making obscene gestures during the lecture and the fear of becoming a male. She had the habit of peeping into the bathroom when her mother takes bath. Sometimes she blamed her mother of appearing nude before her. Her elder sister and elder brother had innocuous relationship. She did not have any intimate relationship with the member of the same sex. The family disapproved of her friendship with boys of questionable character.
译文:
示例案例研究 本科医学论文代写
患者是一名 18 岁的女性,在一所男女同校毕业。 她被母亲和姐姐带到诊所,原因是睡眠不足、言语和身体上的攻击性、怀疑她大学的男教职员工给她写情书并在讲座中做出淫秽手势以及害怕成为男性 . 她有妈妈洗澡时偷看浴室的习惯。 有时她责怪她的母亲裸露在她面前。 她的姐姐和哥哥是无伤大雅的关系。 她与同性成员没有任何亲密关系。 家人不赞成她与性格有问题的男孩的友谊。
Therapeutic Strategies Suggested
The patient mentioned in the case study is suffering from paranoid schizophrenia. In the initial phase of the treatment, she was suggested to undergo neuroleptic pharmacotherapy especially antipsychotic drugs. The medication has been found to be effectual in treating the ‘positive symptoms’ of the disease, the treatment of ‘negative symptoms’ has not very yet found to be very successful. Later on she was suggested to undergo psychotherapeutic interventions like reality-oriented individual therapy so that she could be able to cope up with stressful thoughts and events encountered which eventually reduce the risk for relapse, cognitive-behavioural approach helps in monitoring and changing the negative patterns of thoughts and behaviours in ways to make her able to regulate irrational thoughts and feelings as well as psychosocial therapy such as rehabilitation programme, family therapy in order to enhance her distorted social functioning, coping strategies and problem-solving skills.
译文:
建议的治疗策略 本科医学论文代写
案例研究中提到的患者患有偏执型精神分裂症。在治疗的初始阶段,她被建议接受抗精神病药物治疗,尤其是抗精神病药物。已发现该药物可有效治疗疾病的“阳性症状”,但尚未发现治疗“阴性症状”非常成功。后来她被建议接受心理治疗干预,如面向现实的个体治疗,以便她能够应对遇到的压力想法和事件,最终降低复发的风险,认知行为方法有助于监测和改变消极模式思想和行为的方式,使她能够调节非理性的思想和感觉,以及心理社会治疗,如康复计划、家庭治疗,以增强她扭曲的社会功能、应对策略和解决问题的能力。
The Effect of Individual Psychotherapeutic Intervention
The recent advancement has been observed in the pharmacological management of the psychoses; however, several studies suggest that the prognosis of affective disorder such as psychoses is not up to the mark especially in the cases of relapse (Wiersma et al, 1998; Robinson et al, 1999; Ohmori et al, 1999). Near about 30% of the patients from general population respond poorly to the pharmacological medication with an evidence of persistent symptoms of functional impairment (Kane, 1988). Frangou and Murray (2000) argued that the schizophrenia patients received only pharmacological treatment has shown a limited or insignificant enhancement in social functioning. The implementation of psychiatry has become increasingly categorised into aficionados of the psychodynamic and bio-physiological approaches (Fenton, 2000).

There are different debatable perspectives raised in comparing the value of comprehensive psychotherapeutic intervention versus medication.
However, the past decades has been shifted away from this ideological disputation agreeing that no individual approach could be beneficial in treating schizophrenia, a significant form of psychosis. However, neuroleptic medications are the mainstay in treating psychosis; around 25% – 50% of the victims carry on experiencing unrelenting and distressing symptoms (Garety et al, 2000). 本科医学论文代写
Despite going through thorough medicinal administration, the patients may subject to periodic relapses (Hogarty & Ulrich, 1998). The adherence to medicinal regime may decline due to the unpleasant and disabling side-effects. These primarily prompted many researchers to focus on complementary treatment for psychosis, but yet the comparison between pharmacological studies and psychotherapeutic studies prevailing as the treatment of psychosis describes that there needs to conduct more researches in this area with psychotherapeutic interventions.
Fenton (2000) suggests both a thorough historical account of the theory of individual psychotherapy for schizophrenia and a literature review suggesting its efficacy. He also suggests that there is no individual component that can be accounted for the successful treatment of schizophrenia and an inflexible adherence to an individual technique may lead to the victim in non-beneficial as well as problematic condition (Fenton & McGlashan, 2000). However, researchers have not found any significant correlation among the positive effect derived from the administration of psychodynamic, insight-oriented therapeutic intervention whatsoever (Malmberg & Fenton, 2002).
译文:
个体心理治疗干预的效果 本科医学论文代写
最近在精神病的药物治疗方面取得了进展。然而,一些研究表明,情感障碍(例如精神病)的预后并不理想,尤其是在复发的情况下(Wiersma 等,1998;Robinson 等,1999;Ohmori 等,1999)。一般人群中近 30% 的患者对药物治疗反应不佳,有持续的功能障碍症状的证据 (Kane, 1988)。 Frangou 和 Murray (2000) 认为,仅接受药物治疗的精神分裂症患者在社会功能方面表现出有限或不显着的增强。精神病学的实施越来越被归类为心理动力学和生物生理学方法的爱好者(Fenton,2000)。
在比较综合心理治疗干预与药物治疗的价值时,提出了不同的有争议的观点。
然而,过去几十年已经摆脱了这种意识形态争论,即同意没有任何个人方法可以有益于治疗精神分裂症,这是一种重要的精神病形式。然而,精神安定药物是治疗精神病的中流砥柱。大约 25% – 50% 的受害者继续经历无情和痛苦的症状(Garety 等,2000)。
尽管经过彻底的药物管理,患者可能会定期复发(Hogarty & Ulrich, 1998)。由于令人不快和致残的副作用,对药物治疗的依从性可能会下降。这些主要促使许多研究人员将注意力集中在精神病的补充治疗上,但药理学研究和心理治疗研究之间的比较随着精神病的治疗而盛行,说明需要在该领域进行更多的心理治疗干预研究。
Fenton (2000) 提出了对精神分裂症个体心理治疗理论的全面历史解释和表明其有效性的文献综述。他还表示,没有任何单独的成分可以解释精神分裂症的成功治疗,对个别技术的僵化坚持可能导致受害者处于无益和有问题的状态(Fenton & McGlashan,2000)。然而,研究人员并未发现任何以心理动力学、洞察力为导向的治疗干预所产生的积极影响之间存在任何显着相关性(Malmberg & Fenton,2002)。
Rather they suggest that the possibility of analysing negative effect due to the application of such therapeutic intervention has been ruled out.
Moreover, Fenton (2000) argues that there is little evidence found in the support of the beneficial effect derived from administrating psychodynamic therapy over medication. In the empirical evidence, it has been found that the individuals treated with medication have been shown superior outcomes in comparison with the individuals treated under psychodynamic therapy. Rather it has been found correlated with the patients post-therapeutic impaired functioning as a whole. 本科医学论文代写
On the other hand, psychosocial rehabilitation provides significant add-ons to pharmacotherapy (Bachrach, 2000) which is proven to be beneficial in treating patients suffering from schizophrenia (Bachrach, 1992; Bachrach 1996). The primary objective of this intervention is to facilitate the patients to accomplish the highest possible quality of life by means of regaining the physical, emotional, social and intellectual skills needed to accommodate within the community (Anthony, 1988). However, potential researchers have not yet been conducted in the cases of the individuals with a first episode of psychosis (Huxley, 2000).
译文:
相反,他们认为由于应用此类治疗干预而分析负面影响的可能性已被排除。
此外,Fenton (2000) 认为,几乎没有证据支持精神动力学治疗优于药物治疗。经验证据表明,与接受心理动力学治疗的个体相比,接受药物治疗的个体显示出更好的结果。相反,它被发现与患者治疗后整体功能受损有关。
另一方面,社会心理康复为药物治疗提供了重要的补充 (Bachrach, 2000),已被证明对治疗精神分裂症患者有益 (Bachrach, 1992; Bachrach 1996)。这种干预的主要目标是通过恢复适应社区所需的身体、情感、社交和智力技能,帮助患者实现尽可能高的生活质量(Anthony,1988)。然而,尚未对首次精神病发作的个体进行潜在的研究(Huxley,2000)。
Cognitive Behavioural & Psychosocial Therapeutic Intervention for Psychosis
Cognitive-behavioural approach has been found effective in treating neurotic disorders like anxiety and depression. Hence its application has been increasingly found effective in varied regimes of psychosomatic disorders (Haddock et al, 1998) as well as in the area of treating psychosis. According to Eells (2000), the psychodynamic approach had been contributed largely to the disappointing outcomes which eventually enhance the contribution of comprehensive implementation of psychosocial intervention on psychosis assuming diathesis-stress model in association with the application of pharmacology. Researchers suggest that there is growing evidence that confirm psychotherapeutic interventions such as cognitive-behavioural approach and psychosocial intervention have provided proven benefit and need to undergo extensive evaluation in non-experimental settings (Thornicroft & Susser, 2001). 本科医学论文代写
Tarrier et al (1998a) proposed an investigation for finding out the important improvements in psychotic symptoms and relapse rate intervened by cognitive-behavioural therapeutic interventions.
The study involved cognitive therapeutic assessment as well as supportive counselling to conventional care procedure. The cognitive-behavioural therapeutic intervention included 20 hours of therapeutic session for 10-week period by trained therapists. Both of the groups have been chosen as experienced symptoms for a minimum of past six months. Findings suggest that there is a 50% decline in symptoms along with declined days of staying in hospitals for the control group individuals, assessing which the researchers concluded that cognitive-behavioural therapeutic intervention provided a significant benefit over the conventional one and had been found as potentially beneficial. 本科医学论文代写
However, Curtis (1999) argued that there were no significant differences between the administrations of cognitive-behavioural therapy over conventional counselling with routine care. A follow-up study conducted by Tarrier et al (1999) suggests the potential benefit of cognitive-behavioural therapy over individual supportive counselling especially in the area of reducing positive symptoms of schizophrenia. However, there are no significant differences found between cognitive-behavioural therapy, supportive counselling and routine care in the case of relapse rate. Similarly, the researchers have not found any significant outcomes in the case of negative symptoms while administering cognitive-behavioural therapy or supportive counselling.
译文:
精神病的认知行为和社会心理治疗干预
已发现认知行为方法可有效治疗焦虑和抑郁等神经症。因此,越来越多地发现其在各种心身障碍(Haddock 等,1998)以及治疗精神病领域中的应用是有效的。根据 Eells (2000) 的说法,心理动力学方法在很大程度上导致了令人失望的结果,最终增强了综合实施心理社会干预对假设素质 – 压力模型与药理学应用相关的精神病的贡献。研究人员表示,越来越多的证据表明,认知行为方法和社会心理干预等心理治疗干预措施已被证明具有益处,需要在非实验环境中进行广泛的评估(Thornicroft & Susser,2001 年)。
TARRIER 等人 (1998A) 建议进行一项调查,以找出通过认知行为治疗干预干预的精神病症状和复发率的重要改善。
该研究涉及认知治疗评估以及对常规护理程序的支持性咨询。认知行为治疗干预包括由训练有素的治疗师进行的为期 10 周的 20 小时治疗。两组都被选为在过去六个月内出现症状。研究结果表明,对照组个体的症状减少了 50%,住院天数也减少了,评估研究人员得出结论,认知行为治疗干预比传统干预提供了显着的益处,并且已被发现具有潜在的潜在价值或有利。
然而,Curtis (1999) 认为认知行为疗法与常规咨询和常规护理之间没有显着差异。 Tarrier 等人 (1999) 进行的一项后续研究表明,认知行为疗法优于个体支持性咨询,尤其是在减少精神分裂症阳性症状方面。然而,在复发率的情况下,认知行为疗法、支持性咨询和常规护理之间没有发现显着差异。同样,研究人员在进行认知行为疗法或支持性咨询时没有发现任何阴性症状的显着结果。
In a long-term cognitive-behavioural therapeutic intervention, Wiersma et al (2001) argued about the implementation of the cognitive-behavioural therapy on developing coping skills training on persistent auditory hallucinations and social functioning.
Studies conducted including 40 subjects with duration of four years using several assessment tools such as the Auditory Hallucinations Rating Scale (Haddock, 1994) and the Scale of Positive and Negative Syndrome (Kay et al, 1987) had been found robust effects on hallucinatory complications. However, the study provided numerous limitations as there was neither control group employed nor the assessors were independent. Moreover, the assessment of frequency and subjective burden of voices had been derived in retrospect including a lack of assessing social functioning or psychopathology regarding schizophrenia. 本科医学论文代写
Review of the studies suggest that 18% of the patients came out from the complications of hallucinations whereas 60% of the patients maintained improvement regarding the anxiety, loss of control and impaired thinking pattern, additionally 67% of the patients showed an overall improvement in daily functioning. As suggested by Kuipers et al (1997, 1998) a more comprehensive schema-focused approach involved reflection of the client’s own interpretation of their problems by focusing attention to the development of onset of delusional ideas and hallucinations and its prevalence over time. 本科医学论文代写
The study aimed extensively at the development of coping strategies, problem-solving skills and prevention of relapse in relation to the declining of frequency and severity of psychotic symptoms in association with depression, anxiety, frustration, learned helplessness with an improvement of social functioning, enhancement of self-control of relapse and alternation of dysfunctional schemata. The study conducted by Kingdon and Turkington et al (2000) aimed at providing cognitive-behavioural therapy to reduce distress and disability stemmed from coexisting depression. The researchers concluded that both cognitive-behavioural therapies along with supportive interventions led to clinically significant progress in positive and negative symptoms as the outcomes of the treatment provided.
译文:
在一项长期的认知行为治疗干预中,Wiersma 等人 (2001) 提出了关于实施认知行为疗法的观点,即在持久社会听觉和听觉上发展应对技能培训。
使用几种评估工具(例如幻听评定量表(Haddock,1994)和阳性和阴性综合征量表(Kay 等,1987))对 40 名为期四年的受试者进行了研究,发现对幻觉并发症有强大的影响。然而,该研究存在许多局限性,因为既没有使用对照组,也没有评估人员是独立的。此外,对声音频率和主观负担的评估是回顾性得出的,包括缺乏对精神分裂症的社会功能或精神病理学的评估。
研究回顾表明,18% 的患者从幻觉并发症中解脱出来,而 60% 的患者在焦虑、失控和思维模式受损方面保持改善,另外 67% 的患者在日常工作中表现出整体改善运作。正如 Kuipers 等人 (1997, 1998) 所建议的那样,一种更全面的以图式为中心的方法包括通过将注意力集中在妄想想法和幻觉的发展及其随时间的流行上来反映来访者自己对他们问题的解释。
该研究广泛地针对与抑郁、焦虑、沮丧、习得性无助以及社会功能改善、增强相关的精神病症状的频率和严重程度的下降相关的应对策略、解决问题的技能和预防复发的发展。复发的自我控制和功能障碍图式的交替。 Kingdon 和 Turkington 等人 (2000) 进行的研究旨在提供认知行为疗法,以减少因抑郁症共存而导致的痛苦和残疾。研究人员得出的结论是,认知行为疗法和支持性干预措施均导致阳性和阴性症状在临床上取得显着进展,作为治疗的结果。
Studies suggested that the combination of two treatment approaches like psychotherapeutic interventions along with antipsychotic medication provide more success compared to the single-line approach executed by antipsychotic medication only resulting in more relapse rate for the later (Left and Wing, 1971).
During 1970s and 1980s increasing interests in finding the potential benefit associated with psychosocial intervention suggesting complications in relation to the implementation of single-line treatment of antipsychotic medications focused on four aspects in particular – (1) unpleasant side-effects, (2) persistence of negative symptoms, (3) limitations in social recovery and / or social bankruptcy and (4) deinstitutionalization. 本科医学论文代写
It had been further suggested the significance of family involvement during recovery as well as family’s emotional or attitudinal viewpoint to the recovery of the patient in question in association with the progress in the concept of ‘expressed emotion’ (Linszen et al, 1998). The significance of stress-vulnerability model is reflected through current approaches to the clinical practices and research of psychosocial interventions. Hence the aim of psychosocial intervention is to lessen the effect of environmental stressors on organically vulnerable individuals while endorsing their social involvement and functioning within the community (Falloon et al, 1996).
Neuroleptic pharmacotherapy is used to intervene on the primary symptoms of psychosis such as hallucinations, delusions and thought disorders, on the other hand, psychosocial therapeutics are equally important as they serve to educate, train and rehabilitate the patient to assist in fully functional recovery by means of regaining the capacity for psychological well-being, social and occupational involvement and enhanced quality of life in general.
译文:
研究表明,与抗精神病药物和药物治疗的单线方法相比,将心理治疗干预等两种治疗方法与抗精神病药物相结合可提供更多成功(仅在 R17 中使用抗精神病药物治疗)。
在 1970 年代和 1980 年代,人们越来越有兴趣寻找与心理社会干预相关的潜在益处,这表明与实施抗精神病药物单线治疗相关的并发症特别集中在四个方面——(1)令人不快的副作用,(2)阴性症状,(3)社会恢复和/或社会破产的限制和(4)去机构化。
与“表达情感”概念的进展相关联,有人进一步提出了康复期间家庭参与的重要性以及家庭对患者康复的情感或态度观点(Linszen 等,1998)。压力脆弱性模型的重要性通过当前的临床实践方法和社会心理干预研究得到反映。因此,社会心理干预的目的是减轻环境压力对有机脆弱个体的影响,同时支持他们在社区内的社会参与和功能(Falloon 等,1996)。
抗精神病药物治疗用于干预精神病的主要症状,如幻觉、妄想和思维障碍,另一方面,心理社会治疗也同样重要,因为它们有助于教育、训练和康复患者,通过手段帮助患者完全恢复功能恢复心理健康、社会和职业参与以及提高总体生活质量的能力。
Interventions regarding Acute Psychosis
However, there is not a plenty of research conducted in the area of post-acute, drug-refractory schizophrenia, but still there are studies suggesting that psychotherapeutic interventions may contribute to the recovery from acute psychosis (Grech, 2002). Studies conducted by Drury et al (1996a, 1996b, 2000) suggest the beneficial effect associated with administering cognitive-behavioural therapy in case of acute psychosis by asserting that 35% of the patients experienced long-term outcome of clinical significance (Birchwood et al, 1998; Garety & Jolley, 2000; Drake et al, 2000; Lenior et al, 2001). 本科医学论文代写
The therapeutic interventions were targeted to provide the alteration of delusional beliefs and related distress, improvements in negative symptoms and prevention of relapse. Findings showed that in intervention group 95% of the patients’ modification in positive symptoms was of clinical significance in compared to the 44% of the patients’ in control group. Both of the group showed an improvement in negative symptoms as well. A decline in the delusional conviction had been identified but no significant decline in the preoccupation in the delusional beliefs had been identified. Moreover, the definition of recovery from the acute phase of disorder corresponding to the 25% – 50% decline in the recovery time had been achieved (Drury et al, 1996b).
译文:
关于急性精神病的干预措施 本科医学论文代写
然而,在急性后、药物难治性精神分裂症领域进行的研究并不多,但仍有研究表明心理治疗干预可能有助于急性精神病的康复(Grech,2002)。 Drury 等人 (1996a, 1996b, 2000) 进行的研究表明,通过断言 35% 的患者经历了具有临床意义的长期结果(Birchwood 等人, 1998 年;Garety 和 Jolley,2000 年;Drake 等人,2000 年;Lenior 等人,2001 年)。
治疗干预的目标是改变妄想信念和相关痛苦,改善阴性症状和预防复发。结果表明,干预组 95% 的患者阳性症状改善具有临床意义,而对照组为 44%。两组都显示出阴性症状的改善。已确定妄想信念的下降,但未确定妄想信念的专注度显着下降。此外,已经实现了对应于恢复时间减少 25% – 50% 的疾病急性期恢复定义(Drury 等,1996b)。
Issues involved in working with psychotic patients and their problems
Several studies suggest that there is a significant improvement observed among the patients suffering from schizophrenia if intervened with psychosocial rehabilitation programmes by means of achieving an evident improvement in the quality of life compared to the individuals received only standard care (Whitty, Lydon, Turner & O’Callaghan, 2006) as illustrated in figure 1. The psychosocial rehabilitation programmes facilitate the individuals suffering from psychotic symptoms provide necessary skills for learning and social integration resulting in an improved quality in life style and social functioning as a whole (Bachrach, 1992). However, there are number of issues raised in concern of conducting research in this area of study in essence of ethical, moral, legal and professional terms. 本科医学论文代写
With the introduction of atypical antipsychotic medication it has been clearly illustrated that there is an increase in the annual drug expenditure in a significant fashion (Kleinke, 2000),
however, a significant strain has been put on the annual medical budget due to an escalation of in the medical expenses (Mehl & Santell, 2000), which results in an decline in the services associated with rehabilitation services as these are directed towards the payment for these medications (Baker, 2001). 本科医学论文代写
Moreover, the limitations for conducting psychotherapeutic control group in accordance with psychosocial intervention research may involve complicated ethical issues in terms of consent, confidentiality, boundary violations and risk-benefit issues (Saks et al, 2002). Studies suggest that there is a high satisfaction rate associated with the implementation of cognitive-behavioural therapy along with psychosocial intervention on the patients in general (Kuipers et al, 1997; Kemp et al, 1996, 1998). However, the efficacy of these interventions is largely untested due to inadequate knowledge and insufficient expertise involved during clinical trial (Cormac et al, 2002).
译文:
与精神病患者及其问题一起工作所涉及的问题
几项研究表明,与仅接受标准护理的个体相比,如果通过心理社会康复计划进行干预,精神分裂症患者的生活质量会显着改善(Whitty、Lydon、Turner & O ‘Callaghan, 2006) 如图 1 所示。社会心理康复计划有助于患有精神病症状的个体提供必要的学习和社会融合技能,从而提高生活方式和整体社会功能的质量 (Bachrach, 1992)。然而,在伦理、道德、法律和专业术语的本质上,在这一研究领域进行研究时,存在许多问题。
随着非典型抗精神病药物的引入,它清楚地表明,每年的药物支出显着增加(KLEINKE,2000),
然而,由于医疗费用的增加(Mehl 和 Santell,2000 年),年度医疗预算承受了巨大压力,这导致与康复服务相关的服务减少,因为这些服务直接用于支付这些药物(贝克,2001 年)。
此外,根据社会心理干预研究进行心理治疗控制组的局限性可能涉及同意、保密、边界违规和风险收益问题等复杂的伦理问题(Saks 等,2002)。研究表明,认知行为疗法的实施以及对患者的心理社会干预总体上具有很高的满意度(Kuipers 等,1997;Kemp 等,1996,1998)。然而,由于临床试验期间知识不足和专业知识不足,这些干预措施的有效性在很大程度上未经测试(Cormac 等,2002)。
Conclusion
Several studies are in concordance with the growing evidence of effectiveness in implementing psychotherapy especially benefits associated with cognitive interventions over the non-specific supportive counselling and routine care in association with conventional neuroleptic pharmacotherapy. More explicitly, in the area concerned with symptom-specific approaches relating to the domain of positive symptoms such as delusions and hallucinations, the cognitive behavioural approach along with psychosocial interventions are found to be effective by means of altering dysfunctional schema, improvement in social functioning, problem-solving skills in particular.
译文:
结论 本科医学论文代写
一些研究与越来越多的证据一致,表明实施心理治疗的有效性,尤其是与认知干预相关的益处,而不是与传统精神抑制药物治疗相关的非特异性支持性咨询和常规护理。 更明确地说,在与妄想和幻觉等阳性症状领域相关的症状特异性方法的领域中,发现认知行为方法以及社会心理干预是有效的,方法是改变功能失调的图式、改善社会功能、 尤其是解决问题的能力。
Reference
Saks, E. R., Jeste, D. V., Granholm, B. W., Palmer, B. W. & Schneiderman, L. (2002). Ethical issues in psychosocial interventions research involving controls. Ethics and Behaviour, 12, 87-101.
Baker, J. G. (2001). Engaging community mental health stakeholders in pharmacy cost management. Psychiatric Services, 52(5), 650-653. 本科医学论文代写
Mehl, B., & Santell, J. (2000). Projecting future drug expenditures – 2000. American Journal of Health-System Pharmacy, 57, 129-138.
Kleinke, J. (2000). Just what the HMO ordered: the paradox of increasing drug costs. Health Affairs, 19, 78-91.
Bachrach, L. L. (1992). Psychosocial rehabilitation and psychiatry in the care of long-term patients. American Journal of Psychiatry, 149(11), 1455 –1463.
Bachrach, L. L. (1996). Psychosocial rehabilitation and psychiatry: what are the boundaries. Canadian Journal of Psychiatry, 41(1), 28 – 35.
Bachrach, L. L. (2000). Psychosocial rehabilitation and psychiatry in the treatment of schizophrenia – what are the boundaries. Acta Psychiatrica Scandinavica, 407 (Suppl), 6-10.
Whitty P., Lydon C., Turner N., & O’Callaghan E. (2006). The Influence Of Psychosocial Rehabilitation On Patients With A First Episode Of Psychosis. International Journal of Psychosocial Rehabilitation. 10 (2) 17-27.
Huxley, N. A., Rendall, M. & Sederer, M. (2000). Psychosocial treatments in schizophrenia. A review of the past 20 years. Journal of Nervous and Mental Disease, 188, 187-201. 本科医学论文代写
Anthony, W. A., Cohen, M. R. & Danley, K. S. (1988). The psychiatric rehabilitation approach as applied to vocational rehabilitation. In J. A. Ciardiello (Ed.), Vocational Rehabilitation of Persons with Prolonged Psychiatric Disorders (pp. 224-248). Baltimore: Johns Hopkins University Press.
Frangou, S., & Murray, R. M. (2000). Psychosocial interventions. In S. Fangou (Ed.), Schizophrernia (pp. 61-65). London: Dunitz.
Kane, J., Honigfeld, G., Singer, J. & Meltzer, H. (1988). Clozapine for the treatment-resistant schizophrenic. A double-blind comparison with chlorpromazine. Archives of General Psychiatry, 45, 789-796.
Wiersma, D., Nienhuis, F. J., Sloof, C. J. & Giel, R. (1998). Natural course of schizophrenic disorders: a 15 year follow up of a Dutch incidence cohort. Schizophrenia Bulletin, 24, 75-85.
Robinson, D., Woerner, M. G., Alvir, J. M. Bilder, R., Goldman, R., Giesler S., Koreen, A., Sheitman, B., Chakos, M., Mayerhoff, D. & Lieberman, JA. (1999). Predictors of relapse following response from a first episode of schizophrenia or schizoaffective disorder. Archives of General Psychiatry, 56, 241-7.
Ohmori, T., Ito, K., Abekawa, T. & Koyama, T. (1999). Psychotic relapse and maintenance therapy in paranoid schizophrenia: a 15 year follow up. European Archives of Psychiatry and Clinical Neurosciences, 249, 73-78.
Fenton W.S. (2000). Evolving perspectives on individual psychotherapy for schizophrenia. Schizophrenia Bulletin, 26(1): 47-72. 本科医学论文代写
Garety P.A., Fowler D., Kuipers E., Freeman D., Dunn G., Bebbington P., Hadley C. & Jones S. (1977). London-East Anglia randomised controlled trial of cognitive-behavioural therapy for psychosis. II: predictors of outcome. British Journal of Psychiatry, 171: 420-426.
Fenton, W.S., & McGlashan, T.H. (2000). Schizophrenia: Individual psychotherapy. In: Sadock, B.J., & Sadock, V.A. (eds.) Comprehensive Textbook of Psychiatry, 7th Ed. Philadelphia: Lippencott, Williams & Wilkins. pp.1217-1231.
Malmberg L. & Fenton M. (2002). Individual psychodynamic psychotherapy and psychoanalysis for schizophrenia and severe mental illness (Cochrane Review). In: The Cochrane Library, 1. Oxford: Update Software.
Haddock G., Tarrier N., Spaulding W., Yusupoff L., Kinney C. & McCarthy E. (1998). Individual cognitive-behaviour therapy in the treatment of hallucinations and delusions: A review. Clinical Psychology Review, 18(7): 821-838.
Eells T.D. (2000). Psychotherapy of schizophrenia. Journal of Psychotherapy Practice and Research, 9(4): 250-254.
Thornicroft G. & Susser E. (2001). Evidence-based psychotherapeutic interventions in the community care of schizophrenia. British Journal of Psychiatry, 178: 2-4.
Tarrier N, Yusupoff L, Kinney C, McCarthy E, Gledhill A, Haddock G & Morris J. (1998a). Randomised controlled trial of intensive cognitive behaviour therapy for patients with chronic schizophrenia. British Medical Journal, 317: 303-7.
Tarrier N., Wittkowski A., Kinney C., McCarthy E., Morris J. & Humphreys L. (1999). Durability of the effects of cognitive-behavioural therapy in the treatment of chronic schizophrenia: 12-month follow-up. British Journal of Psychiatry, 174: 500-504.
Curtis D. (1999). Intensive cognitive behaviour therapy for chronic schizophrenia. Specific effect of cognitive behaviour therapy is not proven (Letter). British Medical Journal, 318: 331. 本科医学论文代写
Wiersma D., Jenner J. A., van de Willige G., Spakman M. & Nienhuis F. J. (2001) Cognitive behaviour therapy with coping training for persistent auditory hallucinations in schizophrenia: a naturalistic follow-up study of the durability of effects. Acta Psychiatrica Scandinavica. 103 (5): 393-399
Haddock G. (1994). Auditory Hallucinations Rating Scale (AHRS). Manchester: University of Manchester.
Kuipers E., Garety P., Fowler D., Dunn G., Bebbington P., Freeman D. & Hadley C. (1997). London-East Anglia randomised controlled trial of cognitive-behavioural therapy for psychosis. I: effects of the treatment phase. British Journal of Psychiatry, 171: 319-327. 本科医学论文代写
Kuipers E., Fowler D., Garety P., Chisholm D., Freeman D., Dunn G., Bebbington P. & Hadley C. (1998). London-east Anglia randomised controlled trial of cognitive-behavioural therapy for psychosis. III: Follow-up and economic evaluation at 18 months. British Journal of Psychiatry, 173: 61-68.
Sensky T., Turkington D., Kingdon D., Scott J. L., Scott J., Siddle R., O’Carroll M. & Barnes T. (2000). A randomised controlled trial of cognitive-behavioural therapy for persistent symptoms in schizophrenia resistant to medication. Archives of General Psychiatry, 57: 165-172.
Grech E: Psychological Interventions For Psychosis: A Critical Review Of The Current Evidence. The Internet Journal of Mental Health. 2002.
Drury V., Birchwood M., Cochrane R., & Macmillan F. (1996a) Cognitive therapy & recovery from acute psychosis: a controlled trial. I. Impact on psychotic symptoms. British Journal of Psychiatry, 169: 593-601.
Drury V., Birchwood M., Cochrane R., & Macmillan F. (1996b) Cognitive therapy and recovery from acute psychosis: a controlled trial. II. Impact on recovery time. British Journal of Psychiatry, 169: 602-607.
Drury V., Birchwood M. & Cochrane R. (2000) Cognitive therapy and recovery from acute psychosis: a controlled trial. 3. Five-year follow-up. British Journal of Psychiatry, 177: 8-14.
Birchwood M., Todd P. & Jackson C. (1998). Early intervention in psychosis. British Journal of Psychiatry, 172 (supplement 33): 53-59.
Garety P. & Jolley S. (2000). Early interventions in psychosis. Psychiatric Bulletin, 24: 321-323.
Drake R.J., Haley C.J., Akhtar S. & Lewis S.W. (2000). Causes and consequences of duration of untreated psychosis in schizophrenia. British Journal of Psychiatry, 177: 511-515. 本科医学论文代写
Lenior M.E., Dingemans P.M., Linszen D.H., De Haan L. & Schene A.H. (2001). Social functioning and the course of early-onset schizophrenia: Five- year follow-up of a psychosocial intervention. British Journal of Psychiatry, 179: 53-58
Leff, J., & Wing, J. (1971). Trial of maintenance therapy in schizophrenia. British Medical Journal, 3, 599-604. Cited in Linszen et al., 1998.
Linszen, D.H., Dingemans, P.M.A.J., Scholte, W.F., Lenior, M.E., & Goldstein, M. (1998). Early recognition, intensive intervention and other protective and risk factors for psychotic relapse in patients with first psychotic episodes in schizophrenia. International Clinical Psychopharmacology, 13 (suppl. 1), S7-S12.
Falloon, I.R.H., Coverdale, J.H., & Brooker, C. (1996). Psychosocial interventions in schizophrenia: A review. International Journal of Mental Health, 25 (1), 3-21.
Hogarty G.,& Ulrich R.F. (1998) The limitations of antipsychotic medications on schizophrenia relapse and adjustment and the contributions of psychosocial treatment. Journal of Psychiatric Research, 32: 243–250.
Kay S.R., Fiszbein A. & Opler L.A. (1987). The Positive and Negative Syndrome Scale (PANSS) for schizophrenia. Schizophrenia Bulletin, 13(2): 261–276.
Kemp R., Hayward P., Applewhaite G., Everitt B. & David A. (1996). Compliance therapy in psychotic patients: randomised controlled trial. British Medical Journal, 312: 345-349.
Kemp R., Kirov G., Everitt P., Haywood P., & David A. (1998). Randomized controlled trial of compliance therapy: 18-month follow-up. British Journal of Psychiatry, 172: 413-419.
Kuipers E., Garety P., Fowler D., Dunn G., Bebbington P., Freeman D. & Hadley C. (1997). London-East Anglia randomised controlled trial of cognitive-behavioural therapy for psychosis. I: effects of the treatment phase. British Journal of Psychiatry, 171: 319-327.
Cormac I., Jones C. & Campbell C. (2002). Cognitive behaviour therapy for schizophrenia (Cochrane Review). In: The Cochrane Library, 1. Oxford: Update Software.
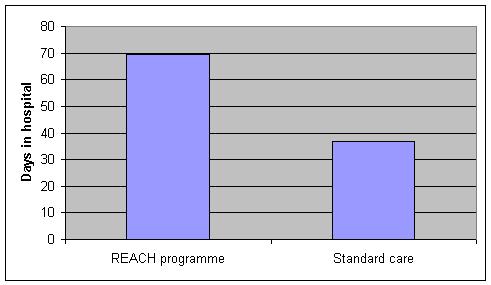
Figure 1: Mean number of days in hospital among patients who completed the REACH programme and those who received standard care
Adopted from Whitty P., Lydon C., Turner N., & O’Callaghan E. (2006). The Influence Of Psychosocial Rehabilitation On Patients With A First Episode Of Psychosis. International Journal of Psychosocial Rehabilitation. 10 (2) 17-27.

其他代写:代写CS C++代写 java代写 matlab代写 web代写 app代写 作业代写 物理代写 数学代写 考试助攻 paper代写 r代写 金融经济统计代写 python代写 英国代写
