Quality Measures In Healthcare And Its Implementation In An Oral Health Organization
(Author’s name)
(Institutional Affiliation)
(Module Title and Number)
(Course Instructor)
(Date of Submission)
(Word count: 3151)
医学论文代写范例 It has also discussed the practices, drivers and procedures to guarantee the quality and safety of the author’s organization.
Abstract
This paper discusses how quality measures influence current practices, dimensions, and drivers for quality and safety in healthcare. Their impact on the delivery of healthcare services in health organizations will also be examined in relation to this. Fundamentally, the paper will provide a description of the structure, delivery of care and quality outcomes to demonstrate how organizations apply safety and quality management principles to guarantee overall patient safety.
Key words: Quality Measures, Oral Health, Patient Safety
译文:
摘要
本文讨论了质量度量如何影响当前医疗保健质量和安全的实践、维度和驱动因素。 它们对卫生组织提供卫生保健服务的影响也将与此相关。 从根本上讲,本文将描述结构、护理交付和质量结果,以展示组织如何应用安全和质量管理原则来保证整体患者安全。
关键词:质量措施,口腔健康,患者安全
Contents 医学论文代写范例
Introduction……………………………………………………………………………………………….2
Structure of the Health Care Organization…………………………………………………….3
Target Population, Clinics and Dental Staff…………………………………………………..3
Figure 1: The organization chart (Source: Author’s organization 2011)…………….4
Delivery of Oral Health Care………………………………………………………………………..4
Health Education………………………………………………………………………………………..5
Prevention………………………………………………………………………………………………….6
Treatment…………………………………………………………………………………………………..8
Safety Measures in Delivery of Care………………………………………………………………10
Quality Control and Outcome Measures………………………………………………………..12
Evaluation of Health Education…………………………………………………………………….13
Evaluation of Preventive Procedures……………………………………………………………..13
Figure 3: Organizational prevention procedures between 2003 and 2010 (Source: Author’s organization 2011)………………………………………………………………………….13
Evaluation of Treatment Procedures……………………………………………………………..14
Continuing dental education:……………………………………………………………………….15
Electronic Health Recoding System (EHRS):…………………………………………………16
Conclusion…………………………………………………………………………………………………16
Introduction
In the last 30 years, various studies have been performed in the field of quality and safety measures in health care with the aim of providing high quality services at affordable cost. These studies have led to an overall change in the understanding of the impact of quality and safety on the outcome of services provided by health care organizations (Groene, O et al. 2010:282). In spite of this change, there is still a debate about how quality can be measured and how it can be improved, given the persistence of quality and safety problems. 医学论文代写范例
Consequently, the focus of the debates have centered on the following factors: safety of patients, effectiveness, timeliness, patient-centered care, efficiency and equity. These elements comprise quality and safety aspects in healthcare and determine the delivery of healthcare services in organizations (Institute of Medicine 200:1). This paper critically discusses how quality measures influence current practices, dimensions, and drivers for quality and safety in healthcare, and their impact on the delivery of healthcare services in health organizations. The discussion will focus on the quality and safety of healthcare in the author’s organization. Subsequent pages will therefore describe the structure, delivery of care and quality outcomes to demonstrate how the organization applies safety and quality management principles to guarantee patient safety.
译文:
介绍
在过去的 30 年中,为了以可承受的成本提供高质量的服务,在卫生保健的质量和安全措施领域进行了各种研究。这些研究导致人们对质量和安全对卫生保健组织提供的服务结果的影响的理解发生了全面变化(Groene,O 等人,2010:282)。尽管有这种变化,鉴于质量和安全问题的持续存在,关于如何衡量质量以及如何改进质量仍然存在争议。医学论文代写例子
因此,争论的焦点集中在以下因素上:患者的安全性、有效性、及时性、以患者为中心的护理、效率和公平。这些要素包括医疗保健中的质量和安全方面,并决定了组织中医疗保健服务的提供 (Institute of Medicine 200:1)。本文批判性地讨论了质量措施如何影响当前医疗保健质量和安全的实践、维度和驱动因素,以及它们对医疗机构提供医疗保健服务的影响。讨论将集中在作者所在组织的医疗保健质量和安全上。因此,后续页面将描述结构、护理提供和质量结果,以展示组织如何应用安全和质量管理原则来保证患者安全。
Structure of the Health Care Organization
The author’s organization provides oral health care services including oral health education, prevention, and treatment to school-aged children. The national level organization was established based on findings of an oral health survey in 1982 showing the need for oral health services for children. The mission of the organization is to decrease the percentage of dental caries (tooth decay) and try to nurture generations through awareness programs on the importance of good oral health.
译文:
卫生保健组织的结构 医学论文代写范例
作者的组织为学龄儿童提供包括口腔健康教育、预防和治疗在内的口腔保健服务。 该国家级组织是根据 1982 年口腔健康调查的结果建立的,该调查结果表明需要为儿童提供口腔健康服务。 该组织的使命是降低龋齿(蛀牙)的百分比,并试图通过有关良好口腔健康重要性的意识计划来培养几代人。
Target Population, Clinics and Dental Staff
The target population for the organization around 300,000 school-going children aged between four and sixteen year. The organization provides oral education, prevention and treatment services in three main clinics: (1) Center-based clinics; (2) School-based fixed clinics; and (3) Mobile clinics (covering schools without fixed clinics) to provide access to dental care for all public school children in the country.
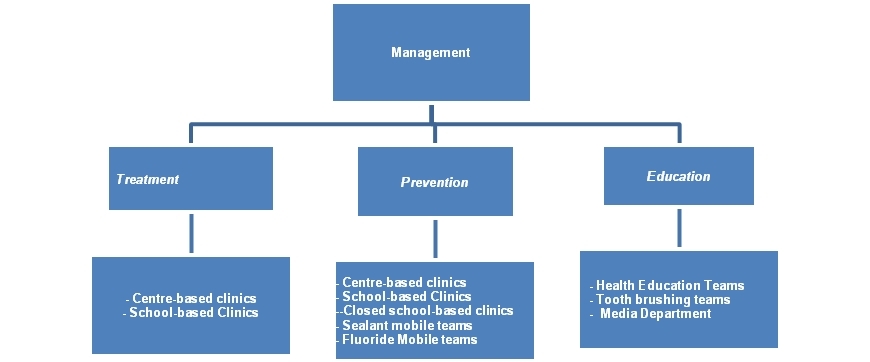
Figure 1: The organization chart (Source: Author’s organization 2011)
Services are similar for all the regions and children. Branches in each governorate are managed by a head that is supported by a Clinical Supervisor (for quality control), prevention leader and health education in-charge. This structure streamlines administrative processes for the smooth flow of operations and quality management.
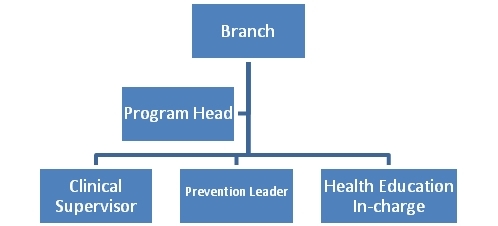
(Source: Author’s organization 2011) Figure 2: Structure at branch level
译文:
目标人群、诊所和牙科工作人员
该组织的目标人群约为 300,000 名 4 至 16 岁的学龄儿童。 该组织在三个主要诊所提供口腔教育、预防和治疗服务:(1) 中心诊所; (2)校本固定诊所; (3) 流动诊所(涵盖没有固定诊所的学校),为该国所有公立学校的儿童提供牙科保健服务。
图 1:组织结构图(来源:作者组织 2011)
所有地区和儿童的服务都是相似的。 每个省的分支机构由一名负责人管理,由一名临床主管(负责质量控制)、预防负责人和健康教育负责人提供支持。 这种结构简化了行政流程,以实现顺畅的运营和质量管理。
(来源:作者组织 2011 年) 图 2:分支机构级别的结构
Delivery of Oral Health Care
There are many opportunities for improving the quality of health care in many hospitals. According to Weiner, Alexander, Shortell, Baker, Becker and Geppert (2006:308), injuries in healthcare organizations are caused by patient exposure to safety risks, issuing wrong prescriptions and lack of follow-up by clinicians in abnormal test results. Consequently, they propose that healthcare organizations implement quality improvement strategies that emphasize continuous improvement of current practices and processes of quality performance. Quality improvement (QI) strategies focus on the practices and processes for quality of healthcare (Bates 2006; Institute of Medicine 200:1). Market concentration and competition from other hospitals, affiliation to system or network, ownership, profitability, inpatient/outpatient ration, hospital size and clinical integration is also important QI strategy (Weiner et al. 2006:310). The QI strategies for the author’s organization are divided into education, prevention and treatment.
译文:
提供口腔保健 医学论文代写范例
许多医院有很多机会可以提高医疗保健质量。根据 Weiner、Alexander、Shortell、Baker、Becker 和 Geppert (2006:308) 的说法,医疗机构中的伤害是由于患者暴露于安全风险、开出错误处方以及临床医生对异常检测结果缺乏跟进而造成的。因此,他们建议医疗保健组织实施质量改进战略,强调持续改进当前的实践和质量绩效流程。质量改进 (QI) 战略侧重于医疗保健质量的实践和过程(Bates 2006;医学研究所 200:1)。市场集中度和来自其他医院的竞争、对系统或网络的从属关系、所有权、盈利能力、住院/门诊量、医院规模和临床整合也是重要的 QI 策略(Weiner 等人,2006:310)。作者组织的QI策略分为教育、预防和治疗。
Health Education
QI strategies on education focus on patient education and practitioner training. Patient education is very important. According to Groene et al. (2010:282), it is the responsibility of healthcare providers to educate the population at a very early stage before the onset of a disease. They claim that it is good practice to collaborate with patients to improve their wellbeing and change their lifestyle from illness to health. An informed patient is an asset to the organization because it reduces cost of treatment and improves the success of the organization’s prevention outcomes. To address patient education issue, the organization implemented an oral health education (OHE) program for children and parents. 医学论文代写范例
OHE is an annual plan that is integrated into school-based education activities and partners with teachers to provide oral education to schoolchildren. The topics should be carefully chosen to meet the needs of children and are managed by education teams who communicate with the students in simple language to make the instructions given more acceptable. Moreover, dentists, dental hygienists or dental assistants use innovative techniques for OHE. Care is taken not to break the local cultural and traditional rules or exceed the limit of understanding of the children. Each centre has specific space for education of children and parents by audio and video means with instructions given mainly by a dental hygienist before the child receives treatment in the clinic. The education teams also reach the families by participating in the social activities to give the instructions about the oral hygiene.
译文:
健康教育 医学论文代写范例
QI 教育策略侧重于患者教育和从业者培训。患者教育非常重要。根据 Groene 等人的说法。 (2010:282),医疗保健提供者有责任在疾病发作之前的早期阶段对人群进行教育。他们声称与患者合作以改善他们的福祉并将他们的生活方式从疾病转变为健康是一种很好的做法。知情患者是组织的资产,因为它可以降低治疗成本并提高组织预防结果的成功率。为了解决患者教育问题,该组织实施了一项针对儿童和家长的口腔健康教育 (OHE) 计划。
OHE 是一项年度计划,它融入校本教育活动并与教师合作,为学童提供口语教育。应仔细选择主题以满足儿童的需要,并由教育团队管理,他们用简单的语言与学生交流,使所给出的指示更容易被接受。此外,牙医、牙科保健员或牙科助理使用创新技术进行 OHE。注意不要打破当地文化和传统规则或超出孩子们的理解范围。每个中心都有专门的空间通过音频和视频方式对儿童和家长进行教育,在儿童在诊所接受治疗之前,主要由牙科保健员进行指导。教育团队还通过参与社会活动来接触家庭,提供有关口腔卫生的指导。
Prevention
The reduction in dental caries had a remarkable progress in the last 30 years because of fluoride use in public water supply, toothpaste and professional dental products; increased access to dental care; and improved oral hygiene (Carounanidy & Sathyanarayanan 2010:209). Studies show that nearly 20 percent of children between 2 and 4 years have detectable dental caries, which increase to 80 percent by 17 years when most of them will have had a cavity manifestation. Moreover, more than 2/3 of adults between 35 to 44 years old will have lost at least one permanent tooth due to dental caries (Carounanidy & Sathyanarayanan 2010:210). 医学论文代写范例
Carounanidy & Sathyanarayanan (2010:210) observe that safety through prevention has been the main changeover of healthcare management.
They note that healthcare providers now focus on preventive strategies and non-invasive illness management. Preventive strategies may be primary, secondary or tertiary. Primary prevention strategies focus on preventing onset of an illness, such as new lesions in dental care, while secondary prevention strategies focus on arresting or controlling the progress of a disease through treatment and lesion management. Tertiary prevention strategies are implemented when the disease has already progressed and focus on administering effective treatment (Carounanidy & Sathyanarayanan 2010:211-12). The author’s organization QI objective is primary and secondary prevention through minimal invasive treatments. The organization has also implemented the following preventive strategies:
- Primary prevention to all children between 4 and 16 years
- Evolving the type and mode of delivery of preventive care
- Performing bi-annual application of FV and FS on newly erupted permanent molars and pre-molars for primary prevention
- Replacing fluoride gel with FV
- Efficient use of portable units to increase prevention productivity
- Increasing mobile clinics to 43 for Sealants and 30 teams for FV application
译文:
预防 医学论文代写范例
由于在公共供水、牙膏和专业牙科产品中使用氟化物,在过去 30 年中减少龋齿取得了显着进展;增加获得牙科护理的机会;和改善口腔卫生(Carounanidy & Sathyanarayanan 2010:209)。研究表明,近 20% 的 2 至 4 岁儿童有可检测到的龋齿,到 17 岁时,这一比例会增加到 80%,届时他们中的大多数都会出现蛀牙。此外,超过 2/3 的 35 至 44 岁成年人将因龋齿而失去至少一颗恒牙(Carounanidy & Sathyanarayanan 2010:210)。
CAROUNANIDY 和 SATHYANARAYANAN (2010:210) 观察到,通过预防实现安全是医疗保健管理的主要转变。
他们指出,医疗保健提供者现在专注于预防策略和非侵入性疾病管理。预防策略可以是一级、二级或三级。一级预防策略侧重于预防疾病的发作,例如牙科护理中的新病灶,而二级预防策略侧重于通过治疗和病灶管理阻止或控制疾病的进展。当疾病已经进展并专注于实施有效治疗时,就会实施三级预防策略(Carounanidy & Sathyanarayanan 2010:211-12)。作者的组织 QI 目标是通过微创治疗进行一级和二级预防。该组织还实施了以下预防策略:
- 所有 4 至 16 岁儿童的一级预防
- 发展预防保健的类型和提供方式
- 对新萌出的恒磨牙和前磨牙每半年应用 FV 和 FS 进行一级预防
- 用 FV 代替氟化物凝胶
- 有效使用便携式装置以提高预防效率
- 将密封剂的流动诊所增加到 43 个,将 FV 应用程序增加到 30 个团队
Carounanidy & Sathyanarayanan (2010:211-212) propose that the organization should use a treatment decision tree to achieve its QI objectives.
The decision tree would help dentist determine the suitability of a preventive treatment for each patient. It would also help them determine the need for intervention, type of treatment (non-operative or operative), treatment regime, minimal restoration, risk status for patients and the dominant causal factors. The decision tree helps practitioners determine whether to progress with application fluoride vanish (FV) or placement of fissure sealants (FS).

FS and FV are used because it reduces dental caries. Adair (2006:134) agrees, ‘FV is a safe material because it helps the teeth to get high concentration of fluoride when applied due to the adhesiveness property and the rate of quality of evidence for the effect of fluoride varnish in preventing and controlling dental caries’. FS uses resin material on teeth to reduce dental carriers. These two measures are useful in reducing dental caries especially in the absence of public water fluoridation (Beauchamp et al. 2008:260; Muller-Bolla, Lupi-Pequrier, Tardieu, Velly and Antomarchi 2006: 323). 医学论文代写范例
Although a preventive decision tree is effective for QI, practitioners find it challenging to implement patient safety strategies for all children through school-based, mobile or centre clinics. Weiner et al. (2007) believes that this problem is due to dilution of focus between the clinics and the hospital, which cause management to engage in diverse and unrelated QI projects. Moreover, separating QI between the hospitals and clinics means that management and staff have to split resources and attention among each QI project and spread the resources too thinly. Therefore, it is paramount that the organization integrates clinic and hospital quality strategies to ensure equity, timeliness, acceptability, effectiveness, and patient-centered care (Maxwell 1992:171).
译文:
CAROUNANIDY & SATHYANARAYANAN (2010:211-212) 建议组织应该使用治疗决策树来实现其 QI 目标。
决策树将帮助牙医确定对每位患者进行预防性治疗的适用性。它还将帮助他们确定干预的必要性、治疗类型(非手术或手术)、治疗方案、最低限度的恢复、患者的风险状况和主要的因果因素。决策树可帮助从业者确定是使用氟化物清漆 (FV) 还是使用窝沟封闭剂 (FS)。
使用 FS 和 FV 是因为它可以减少龋齿。 Adair (2006:134) 同意,’FV 是一种安全的材料,因为它的粘附性和氟化物清漆在预防和控制牙病方面的效果的证据质量在使用时有助于牙齿获得高浓度的氟化物。龋齿’。 FS 在牙齿上使用树脂材料以减少牙科载体。这两种措施可用于减少龋齿,尤其是在没有公共饮水氟化的情况下(Beauchamp 等人 2008:260;Muller-Bolla、Lupi-Pequrier、Tardieu、Velly 和 Antomarchi 2006:323)。
尽管预防决策树对 QI 有效,但从业者发现通过学校、流动或中心诊所为所有儿童实施患者安全策略具有挑战性。韦纳等人。 (2007) 认为,这个问题是由于诊所和医院之间的注意力分散,导致管理层从事多样化和不相关的 QI 项目。此外,医院和诊所之间的 QI 分离意味着管理层和员工必须在每个 QI 项目中分配资源和注意力,资源分散得太细。因此,组织整合诊所和医院质量策略以确保公平、及时、可接受、有效性和以患者为中心的护理至关重要(Maxwell 1992:171)。
Treatment
There is a high percentage of dental caries incidences especially among young population in the Middle East, which has affected the quality and delivery of treatment in the organization. Moreover, the high treatment costs and government sponsoring which make it a right for all children to access free dental care has affected the organization’s service quality. Presently, the organization offers five key treatments including restoration of decayed/broken down teeth; pulpotomy and stainless steel crowns for primary teeth; pulpotomy and pulpectomy for permanent teeth; extraction for badly decade teeth and patient referrals. 医学论文代写范例
To ensure patient safety, treatment is given only in centre- and fixed school-based clinics, as the procedures are critical and need to be done in a specific environment with strict infection control measures.
The Institute of Medicine (2001:2) posits that reinventing the system at treatment level could improve the quality and delivery of health care. This reinvention can be implemented by reengineering care processes, using information technologies effectively, managing knowledge and talent, developing effective teams and coordinating care across patients, services and location of clinics. It proposes the following ten principles to support the redesign:
- Ensuring that care focuses on establishing healing relationships with patients by being responsive at all times via telephone, Internet, mobile clinics and school visits.
- Customizing care according to the needs and values of the patient
- Giving patients the necessary information and opportunity to control their healthcare decisions through shared decision-making with the caregiver
- Sharing information with patients and encouraging open communication between patients and clinicians. 医学论文代写范例
- Ensuring that decisions are evidence-based so that care from clinicians relies on scientific knowledge
- Implementing patient safety to keep patients safe from injury, reduce risks and mitigate practitioner errors.
- Ensuring transparency by making the system available to patients, their families and clinicians so that the safety and satisfaction of patients is achieved.
- Anticipating the needs of the patients instead of reacting to events
- Decreasing the waste of resources or patient time
- Facilitating clinician and institutional cooperation through information exchange, collaboration and care coordination (Institute of Medicine 2001:4).
译文:
治疗 医学论文代写范例
龋齿发生率很高,尤其是在中东的年轻人中,这影响了组织的治疗质量和提供。此外,高昂的治疗费用和政府资助使所有儿童都有权获得免费牙科护理,这影响了该组织的服务质量。目前,该组织提供五种主要治疗方法,包括修复腐烂/折断的牙齿;乳牙的牙髓切断术和不锈钢牙冠;恒牙的牙髓切开术和牙髓切除术;拔牙严重十年和病人转诊。
为确保患者安全,仅在中心和固定的学校诊所进行治疗,因为程序至关重要,需要在具有严格感染控制措施的特定环境中进行。
医学研究所 (2001:2) 认为,在治疗层面重塑系统可以提高医疗保健的质量和提供。可以通过重新设计护理流程、有效使用信息技术、管理知识和人才、发展有效团队以及协调患者、服务和诊所位置的护理来实施这种重塑。它提出了以下十项原则来支持重新设计:
- 确保护理的重点是通过电话、互联网、移动诊所和学校访问随时响应,与患者建立治愈关系。
- 根据患者的需求和价值观定制护理
- 通过与护理人员共享决策,为患者提供必要的信息和机会来控制他们的医疗保健决策
- 与患者共享信息并鼓励患者与临床医生之间的公开交流。
- 确保决策以证据为基础,以便临床医生的护理依赖于科学知识
- 实施患者安全以保护患者免受伤害,降低风险并减少从业者的错误。
- 通过将系统提供给患者、他们的家人和临床医生来确保透明度,从而实现患者的安全和满意度。
- 预测患者的需求而不是对事件做出反应
- 减少资源或患者时间的浪费
- 通过信息交流、协作和护理协调促进临床医生和机构的合作(医学研究所 2001:4)。
Safety Measures in Delivery of Care
Numerous safety controls have been introduced in author’s oral health care organization to ensure the safety of the child, operator, and the procedures performed. Some of them are listed below:
- Consent – Requires the organization to create separate consent forms for prevention and treatment procedures in local language and signed by parents.
- Insurance policies – To protect the child and staff from malpractice, liabilities, workman compensation among other patient-related risks. 医学论文代写范例
- Referral centers – To establish networks with adequate referral centers that can take over any complications or emergencies
- Infection control procedures – To implement infection control measures to ensure the safety of patients and staff.
- Post-operative care- To specify strategies for post-operative care and ensure patient satisfaction
- Emergency clinics – The organization should have an emergency clinic offering emergency services that extend to the holidays.
- Digital radiography – Proposes the use digital radiographs that limit child exposure to about 70 percent compared to conventional radiographs
Practitioner training is an important safety measure.
The author’s organization training ensures that the dentists diagnose dental caries properly and make the right decision on the most appropriate treatment. Dentists should be trained on the treatment decision tree to help them determine whether intervention is needed, what type of treatment to use (non-operative or operative), the regimen, minimal restoration, patient’s risk status, and the dominant causal factors (Carounanidy & Sathyanarayanan 2010:211-212). Employee safety is also important. This is because health care providers are exposed infections like Hepatitis BV (HBV) or Human Immuno deficiency Virus (HIV) and many other micro organisms which can be fatal or destroy the career of the health care worker if the patient got an infection in the clinic (Suñol et al. 2009:i59). Therefore, all the procedures in the organization should follow the guidelines given by Center for Disease Control (CDC). 医学论文代写范例
Groene et al. (2010) posit that standardization of processes a key factor influencing QI. They suggest that all of the treatment procedures should be standardized in a clinical protocol, which is regularly updated to meet technological and evidence-based demands. The standards emphasize early diagnosis and treatment, and the use of minimally invasive techniques. Moreover, treatment procedures should be performed on quadrant basis in order to finish as much treatment in single appointment and high patient to practitioner ratios. Accreditation is another safety measure (Legido-Quigley et al. 2008).
And it is planned to be for the author’s organization in order to improve service delivery.
All employees have to wear protective masks, face shields, eyeglasses and protective clothing while working in clinics or sterilization room. Gloves are changed for every patient and used only once. The surfaces of the dental units and clinics are disinfected after finishing the procedure, and hand wash is mandatory before and after working on patients. Instruments and hand pieces used during each procedure should be washed and cleaned thoroughly to remove all residual materials,
The oral health organization sterilization room is divided into three areas:
- Area of Receiving and washing the contaminated instruments
- Area of Packing and sterilizing by autoclaves
- Area of production clean sterilized instruments.
After sterilization, instruments should be bagged until the next use or expiry of sterilization period (month from the date of sterilization). The packages are then stamped to show the sterilization date on the package. If package is opened for any reason, instruments are cleaned and sterilized again. The clinical supervisor or infection control personnel monitor these safety policies to guarantee the quality of safety and infection control measures. Employees working in the sterilization room should be well trained in washing the instruments, using autoclaves, signing the checklist of sterilization circles and the checklist of the received and delivered instruments. The employees in the sterilization area are reworded for their work in a critical area in the author’s organization.
译文:
提供护理的安全措施 医学论文代写范例
在作者的口腔保健组织中引入了许多安全控制措施,以确保儿童、操作者和所执行程序的安全。其中一些如下所列:
- 同意书——要求组织以当地语言为预防和治疗程序创建单独的同意书,并由父母签署。
- 保险单——保护儿童和员工免受医疗事故、责任、工人赔偿以及其他与患者相关的风险。
- 转诊中心 – 建立具有足够转诊中心的网络,可以接管任何并发症或紧急情况
- 感染控制程序——实施感染控制措施以确保患者和员工的安全。
- 术后护理 – 指定术后护理策略并确保患者满意度
- 急诊室——组织应该有一个急诊室,提供延伸至假期的急诊服务。
- 数字射线照相 – 建议使用数字射线照相,与传统射线照相相比,将儿童暴露在 70% 左右
从业人员培训是一项重要的安全措施。
作者的组织培训确保牙医正确诊断龋齿,并就最合适的治疗做出正确的决定。牙医应该接受治疗决策树的培训,以帮助他们确定是否需要干预、使用哪种治疗类型(非手术或手术)、方案、最小修复、患者的风险状态以及主要的因果因素(Carounanidy & Sathyanarayanan 2010:211-212)。员工安全也很重要。这是因为医疗保健提供者暴露于感染,如乙型肝炎病毒 (HBV) 或人类免疫缺陷病毒 (HIV) 和许多其他微生物,如果患者在诊所感染,这些微生物可能会致命或破坏医疗保健工作者的职业生涯(Suñol 等人,2009:i59)。因此,组织中的所有程序都应遵循疾病控制中心 (CDC) 给出的指导方针。
格罗内等人。 (2010) 假定流程标准化是影响 QI 的关键因素。他们建议所有治疗程序都应在临床方案中标准化,该方案会定期更新以满足技术和循证需求。该标准强调早期诊断和治疗,以及使用微创技术。此外,治疗程序应该在象限基础上进行,以便在一次预约中完成尽可能多的治疗和高患者与医生的比例。认证是另一种安全措施(Legido-Quigley 等人,2008 年)。
并且计划供作者的组织使用,以改进服务交付。
所有员工在诊所或消毒室工作时,必须佩戴防护口罩、面罩、眼镜和防护服。为每位患者更换手套并且仅使用一次。牙科治疗室和诊所的表面在完成程序后进行消毒,并且在为患者工作之前和之后必须洗手。在每个程序中使用的器械和手柄应彻底清洗和清洁,以去除所有残留材料,
口腔卫生组织灭菌室分为三个区域:
- 接收和清洗受污染仪器的区域
- 高压灭菌器包装和灭菌区域
- 生产区清洁消毒器械。
灭菌后,器械应装袋直至下次使用或灭菌期(自灭菌之日起的一个月)届满。然后在包装上盖章以在包装上显示灭菌日期。如果由于任何原因打开包装,器械将再次清洁和消毒。临床主管或感染控制人员监控这些安全政策,以保证安全和感染控制措施的质量。在灭菌室工作的员工应接受器械清洗、使用高压灭菌器、签署灭菌圈检查表和收到和交付的器械检查表等方面的培训。灭菌区域的员工因在作者组织的关键区域工作而被改写。
Quality Control and Outcome Measures 医学论文代写范例
Quality control through supervision is very important in an organization because it monitors the implementation of quality and safety strategies (Legido-Quigley et al. 2008; Stockmeier & Clapper 2011). Senior staff should perform the supervision to evaluate the quality of procedures. Some of the evaluation procedures in the author’s organization are:
Evaluation of Health Education
The performance of education teams is monitored and evaluated by a monthly reporting to the team leaders and program administration, which gives an idea about who, what was done and where. The information given is followed up and evaluated by health education department in order to assure the quality of procedures. In addition, the outcome of educational programs is measured on regular basis by conducting Knowledge, Attitude and Practice surveys on the selected population.
Evaluation of Preventive Procedures
Quantitatively, the productivities of the work done measured on daily basis which are later summarized on weekly, monthly, semi-annual and annual basis. Quality measurements of the preventive fillings (Sealants) placed is done on monthly and annual basis. Outcome of the fluoride program is evaluated by measuring the disease levels in a selected sample of children and comparing the results with controls. Some of the quantitative and qualitative measures for prevention performed under this organization are depicted in the graphs below:
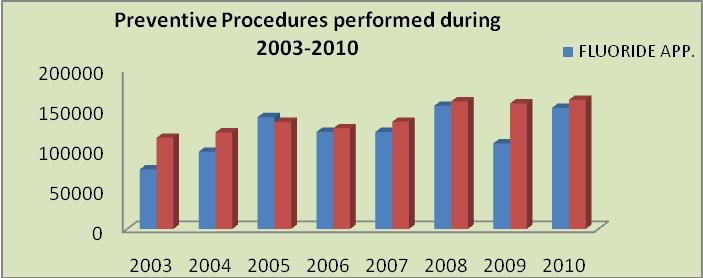
Figure 3: Organizational prevention procedures between 2003 and 2010 (Source: Author’s organization 2011)
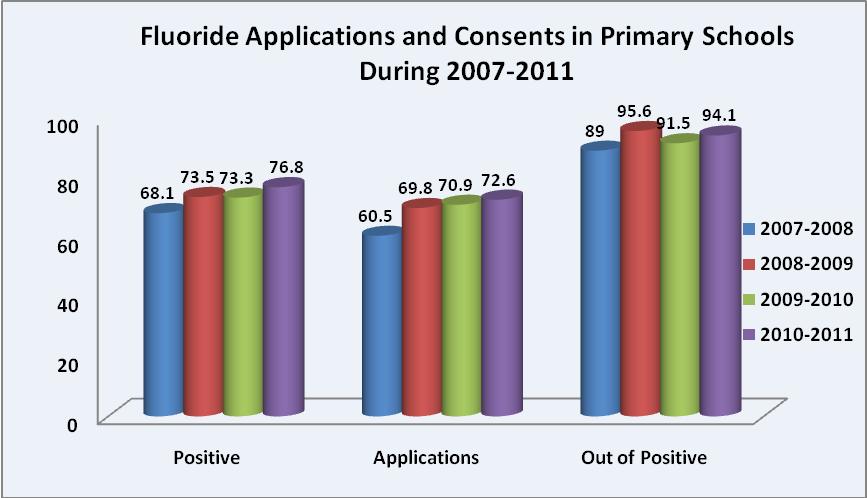
Figure 4. Increase in fluoride applications and consents in primary schools between 2007 and 2011 (Source: Author’s organization 2011)
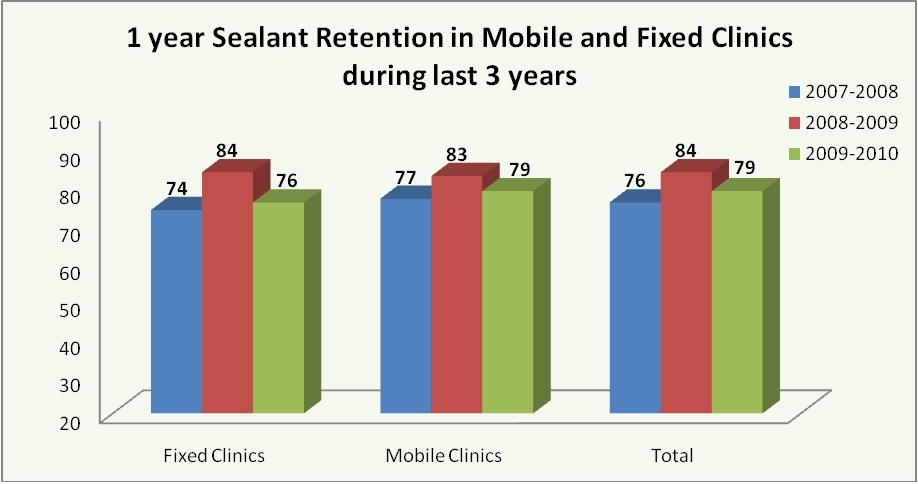
. figure 5:Trends in sealant retention in mobile and fixed clinics for the last 3 years (Source: Author’s organization 2011)
Evaluation of Treatment Procedures
Quality of the procedures performed should be performed on a regular basis (Adair 2006:137) while staff should be evaluated on an annual basis. proposes that overall outcome measures in terms of disease levels be measured once in 5 years in patients.
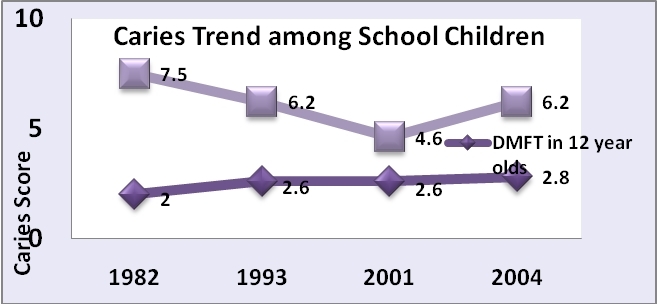
Figure 6: Five-year measures of caries trend in schoolchildren (Source: Author’s organization2011)
Two important measures employed by this organization for improving the quality of care provided are:0
译文:
质量控制和结果测量 医学论文代写范例
通过监督进行的质量控制在组织中非常重要,因为它监控质量和安全战略的实施(Legido-Quigley 等人,2008 年;Stockmeier & Clapper 2011 年)。高级人员应进行监督以评估程序的质量。作者组织中的一些评估程序是:
健康教育评估
教育团队的绩效通过每月向团队领导和项目管理人员报告的方式进行监控和评估,从而了解谁、做了什么以及在哪里完成。提供的信息由健康教育部门跟进和评估,以确保程序的质量。此外,通过对选定人群进行知识、态度和实践调查,定期衡量教育计划的结果。
预防程序的评估
在数量上,每天测量完成的工作的生产力,然后每周、每月、每半年和每年汇总。放置的预防性填充物(密封剂)的质量测量每月和每年进行一次。氟化物计划的结果是通过测量选定儿童样本的疾病水平并将结果与对照组进行比较来评估的。在该组织下执行的一些定量和定性预防措施如下图所示:
图 3:2003 年至 2010 年的组织预防程序(来源:作者组织 2011)
图 4. 2007 年至 2011 年小学氟化物应用和同意的增加(来源:作者组织 2011)
.图 5:过去 3 年流动和固定诊所的密封剂保留趋势(来源:作者组织 2011)
治疗程序的评估
所执行程序的质量应定期执行(Adair 2006:137),同时应每年对员工进行评估。建议在患者中每 5 年测量一次疾病水平方面的总体结果指标。
图 6:学童龋病趋势的五年测量值(来源:作者组织 2011)
该组织为提高所提供的护理质量而采用的两项重要措施是:0
Continuing dental education:
Continuous dental education has a great role in the author’s organization for all the staff, covering wide range of topics. Poortermaan, & Eijkman (1998:346) concur that it is responsibility of the practitioner to update his knowledge and skill level to practice dentistry properly. This explains why it is mandatory for the concerned staff to attend continuous education for professional growth. Dutch National Council for Public Health has established ‘aspect approach’ dividing quality into various aspects: quality of treatment; quality of professional attitude; and quality of the professional organization (National Institutes of Health 2001). These three divisions can be fulfilled by continuous education, training, and planning based on community needs with clinics can be accessed by most of the target population with putting into consideration the culture of society and the life style.
译文:
继续牙科教育:
持续的牙科教育在作者对所有员工的组织中发挥了重要作用,涵盖了广泛的主题。 Poortermaan, & Eijkman (1998:346) 一致认为,从业者有责任更新他的知识和技能水平以正确地实践牙科。 这解释了为什么相关员工必须参加职业发展的继续教育。 荷兰国家公共卫生委员会建立了“方面方法”,将质量分为多个方面:治疗质量; 职业态度的品质; 和专业组织的质量(美国国立卫生研究院 2001)。 这三个部门可以通过基于社区需求的持续教育、培训和规划来实现,大多数目标人群都可以访问诊所,同时考虑到社会文化和生活方式。
Electronic Health Recoding System (EHRS):
Electronic Health Recording System (EHRS) is part of the structure and process of care as it improves the collection and storage of data. The outcome of EHRS depends on the level of security can be given on the aspect of accessing the data and the benefits that can be gained from facilitating communication among health care providers and between health care providers and patients (Int J Med Inform. 2006; Aspeder, Corrigan, Cot 2004). This system makes data entry and analysis efficient, and less time consuming. However, the main challenge for most organizations is profiling dental providers through electronic records (Hassan 2005). Training users on the system functions can solve this challenge. EHRS has gone a long way in improving the quality of care and making organizations more patient-centered.
译文:
电子健康记录系统 (EHRS):
电子健康记录系统 (EHRS) 是护理结构和流程的一部分,因为它改进了数据的收集和存储。 EHRS 的结果取决于在访问数据方面可以提供的安全级别以及通过促进医疗保健提供者之间以及医疗保健提供者与患者之间的沟通可以获得的好处(Int J Med Inform. 2006; Aspeder , Corrigan, Cot 2004)。 该系统使数据输入和分析更加高效,而且耗时更少。 然而,大多数组织面临的主要挑战是通过电子记录对牙科提供者进行分析(Hassan 2005)。 对用户进行系统功能培训可以解决这一挑战。 EHRS 在提高护理质量和使组织更加以患者为中心方面取得了长足的进步。
Conclusion
This paper has discussed quality measures in health care. It has also discussed the practices, drivers and procedures to guarantee the quality and safety of the author’s organization. The organizational structure shows delivery of care centered on leadership, commitment and teamwork. The author’s organization has established strategies for quality improvement through networking between centers and clinics (fixed and mobile), affiliation to system or leadership and clinical integration The quality improvement strategies are divided into education, prevention and treatment. Overall safety measures for quality delivery in the organization include consent, insurance policies, referral centers, infection control procedures, post-operative care and emergency clinics. Quality control and evaluation measures are also performed to ensure quality care. Further research on quality and safety management in dental practice is needed to improve service delivery for the children.
译文:
结论 医学论文代写范例
本文讨论了卫生保健中的质量措施。 它还讨论了保证作者组织的质量和安全的实践、驱动因素和程序。 组织结构显示提供以领导力、承诺和团队合作为中心的护理。 作者的组织已通过中心和诊所(固定和移动)之间的联网、隶属于系统或领导层以及临床整合制定了质量改进策略。质量改进策略分为教育、预防和治疗。 组织内质量交付的整体安全措施包括同意、保险单、转诊中心、感染控制程序、术后护理和急诊室。 还执行质量控制和评估措施以确保质量护理。 需要进一步研究牙科实践中的质量和安全管理,以改善为儿童提供的服务。
References 医学论文代写范例
Adair, S. 2006, ‘Evidence-based Use of Fluoride in Contemporary Pediatric Dental Practice’, Pediatric Dentistry, vol. 28, No. 2, pp. 133-142.
Aspeder, I., Corrigan, J. & Wol C. eds. 2004, Patient Safety: Achieving a New Standard for Care, National Academies Press, Washington DC.
Bates, D.W. 2006, The Safety and Quality of Health Care, Viewed 2 February 2012, http://www.aihw.gov.au/safety-and-quality-of-health-care/
Beauchamp, J., Page C., James C., Kevin D., Robert F., Barbara G., Amid I., William K., Mark S., & Richard S. 2008, ‘Evidence-based Clinical Recommendations for the Use of Pit-and-Fissure Sealants: A report of the American Dental Association Council on Scientific Affairs’, JADA vol. 139, pp. 257-268.
Carounanidy, U., & Sathyanarayanan, R. 2010, ‘Dental Caries: A Complete Changeover, Part III: Changeover in the Treatment Decisions and Treatments’, Journal of Conservation Dentistry, vol. 13, No. 4, pp. 209-217.
Groene, O., Niek K., Cordula W., Onyebuchi A., Andrew T., Charles B., & Rosa S. 2010, ‘Investigating Organizational Quality Improvement Systems, Patient Empowerment, Organizational Culture and the Quality of Care in European Hospitals: The ‘Deepening our Understanding of Quality Improvement in Europe (DUQuE) project’, BMC Health Services Research, vol.10, pp. 281-291.
Hassan, A. H. 2005, Quality Assurance of Dental Health Services provided at the Faculty of Dentistry, King Abdulaziz University.
Institute of Medicine. 2001, Crossing the Quality Chasm: A New Health System for 21st Century, National Academy Press, Washington.
Int J Med Inform. 2006, Definition, Structural, Content, Use and Impact of Electronic Health recourses: A View of the Research Literature.
Legido-Quigley, Martin M., Kieran W., Rosa S., Ellen N., & Niek K. 2008, ‘How Can Quality of Health Care Be Safeguarded Across the European Union’, British Medical Journal, vol. 336, no. 7650, pp. 920-923.
Maxwell, R. J. 1992, ‘Dimension of Quality Revisited: From Thoughts to Action’, Quality Health Care, vol. 1, no. 3, pp. 171-177.
Muller-Bolla M., Lupi-Pequrier L., Tardieu C., Velly A., & Antomarchi C. 2006. ‘Retention of Resin-based Pit and Fissure Sealants: A Systematic Review’, Community Dentistry Oral Epidemiology, vol. 34, no. 5, pp. 321-336.
National Institutes of Health 2001, ‘NIH Consensus Development Conference on Diagnosis and Management of Dental Caries throughout life’, 26-28 March, Bethseda, Maryland.
Poortermaan, J., Carolien W. & Michiel E. 1998. ‘Quality Assurance in Dentistry: The Dutch Approach’, International Journal for Quality in Health Care, vol. 10, no. 4, pp. 345-350.
Stockmeier, Carole, and Craig Clapper. 2011, ‘Daily Check-in for Safety: From Best Practice to Common Practice’, Patient Safety & Quality Healthcare, Viewed 2 February 2012, http://www.psqh.com/septemberoctober-2011/980-daily-check-in-for-safety-from-best-practice-to-common-practice.html.
Suñol, R., Vallejo P., Thompson A., Lombarts M., Shaw C., & Klazinga N. 2009, ‘Impact of Quality Strategies on Hospital Outputs’, Quality Safety Health Care, vol. 18, pp. i62-i68.
Suñol, R., Vallejo P., Groene O., Escaramis G., Thompson A., Kutryba B. & Garel P. 2009, ‘Implementation of Patient Safety Strategies in European Hospitals’, Quality Safety Health Care vol. 18, no. 1, pp. i57-i61.
Weiner B., Jeffrey A., Shortell S., Baker L., Becker M., & Geppert J. 2006, ‘Quality Improvement Implementation and Hospital Performance on Quality Indicators’, Health Services Resolution, vol. 41, no. 2, pp. 307-334.

更多代写:Web开发代写 Management期末考试代考 研究报告代写 英国case study作业代写 math论文代写 英国online exam代考
